

About Us
We are happy to announce the BestOne Dental Plans that are designed for individuals and/or families to maintain good dental hygiene at a very affordable price – healthy mouth, healthy body!
These plans are unique, competitively priced and provide extremely generous benefits. Maximum benefits are available up to $5,000 per calendar year, per covered person, issued to age 99! The PPO dental network combines two national dental networks, enabling us to broaden the availability of dental providers to our customers. The primary PPO Dental network serves over 20 Million members. Coverage is accepted at over 442,000 dental locations.
With BestOne Dental, Customers have seen Savings of up to 50% compared to similar products.* *Refers to premiums paid vs similar individual dental products.
Call us today at 800-454-1021 for more information & details on these exciting new Dental Plans!

Coverage Options
CHOICE PLAN OPTION
$3,000 OR $5,000

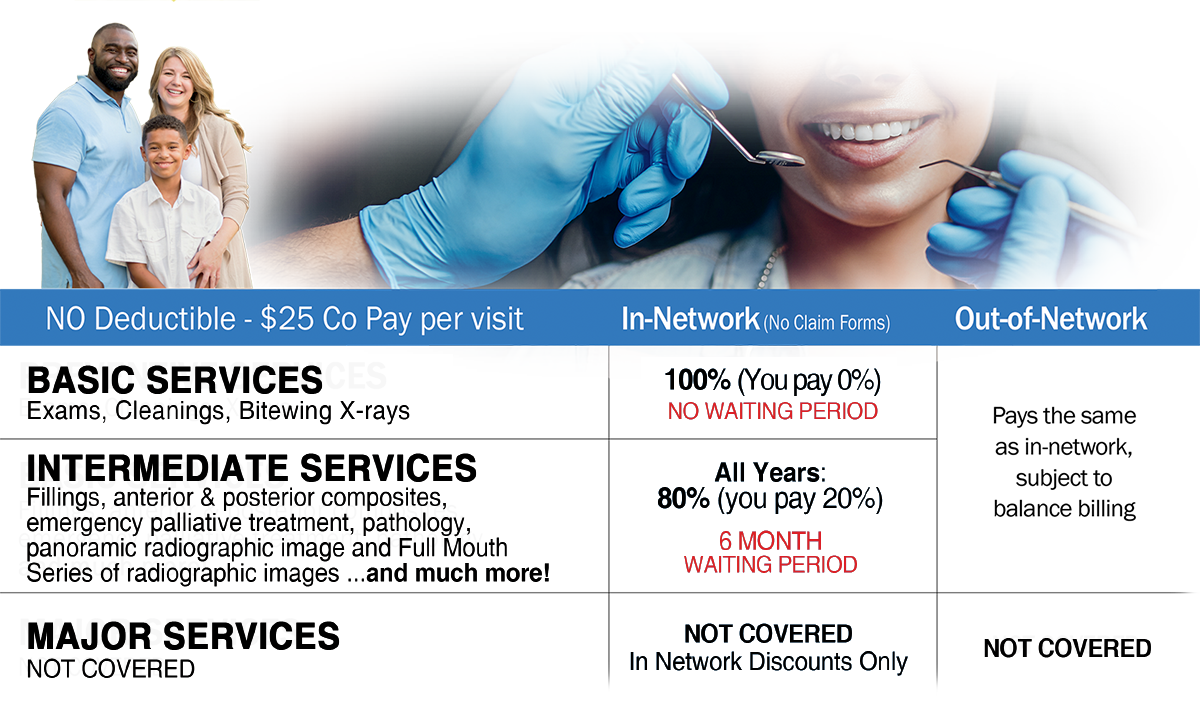
✔ NO Waiting Period & NO Deductible
✔ *$25 Copay Per Visit
✔ Implants Covered on Major Services
✔ No Claim Forms In Network
Certain services include limitations; see Policy for details. 1Implants covered on same benefit schedule as a fixed prosthetic. *Coinsurance applies on certain procedures.

ECONOMY PLAN OPTION - $1,500
$1,500 Max Benefits, Per Calendar Year, Available Ages 18-99, for Individuals and/or Families.
The Best One Dental Economy Plan is an affordable great choice when looking for dental coverage.
✔ NO Waiting Period for Basic Services
✔ Rates Remain as of Issue Age
✔ 2 Large National PPO Networks
✔ 6 Month Waiting Period on Intermediate Services

Basic Covered Services
(Choice Plan & Economy Plan Options)
Basic
✔ Prophylaxis – adult and covered children; once every six months
✔ Topical fluoride – two per twelve months for covered children age 19 and under
Diagnostic
✔ Oral evaluations; one every six months
✔ Comprehensive periodontal evaluations; one every six months
✔ Bitewing X-rays; one set every twelve months
✔ Vertical bitewings; one set every twelve months

Intermediate Covered Services
(Choice Plan & Economy Plan Options)
Diagnostic & Treatment Services
✔ Palliative (emergency) treatment of dental pain
Restorative
✔ Amalgam, primary or permanent & resin-based composite
✔ Sealants – once every sixty months for 1st and 2nd molars only
Major Covered Services
(Choice Plan Option)
Restorative & Crowns
✔ Inlays , onlays and recementing
✔ Crowns; cast posts and core buildups
✔ Pin retention in addition to restoration
✔ Crown repair due to restorative material failure
Gingivectomy or gingivoplasty
✔ Gingival flap procedure
✔ Osseous surgery
✔ Periodontal scaling and root planing – one every thirty-six months
✔ Full-mouth debridement to enable comprehensive evaluation and diagnosis
✔ Periodontal maintenance – one every thirty-six months per individual
Prosthodontics
✔ Gingival flap procedure
✔ Complete and partial dentures – once every seven years for complete dentures to replace missing/broken teeth
✔ Adjustment and repair of dentures
Implants
✔ Limited to one in a lifetime per site and covered as an alternative to a fixed prosthetic only
✔ Cost of fixed prosthetic will be applied to the total value of the implant and implant-related services, not to exceed the cost of the fixed prosthetic
Dental Provider Lookup
The PPO dental network combines two national dental networks, DenteMax and Connection Dental, enabling us to broaden the availability of dental providers to our customers. The primary PPO Dental network serves over 20 million members. Coverage is accepted at over 442,000 dental locations.
CLICK HERE or on the image below and enter your location to find a network dentist near you.
800-454-1021
Frequently Asked Questions

For general questions, please send us a message and we'll get right back to you. You can also call us directly to speak with a member of our service team. 800-454-1021
-
Is there a waiting period for coverage?
There is No waiting period on the Choice Plan $3000 and $5000 annual maximum options. There is No waiting period on the Economy Plan $1500 annual maximum option for Basic Services but there is a 6 month waiting period for Intermediate Services.
-
Are there any Networks?
Yes. Our National Networks of Dentemax and Connection Dental have over 20 million members and over 265,000 Provider Access Points.
-
Is children's coverage same as adults?
Yes – Each covered child has the same annual maximum and benefits as the covered adults.
-
Does Best One Dental cover implants?
Yes. Please see brochure for details.CLICK HERE TO VIEW BROCHURE
-
Are there any Deductibles?
There are No Deductibles, only a $25 co-pay per visit. Coinsurance applies on certain procedures.
-
Are claim forms required?
No claim forms required when using in-network dentists. If you were to go out of network then claim forms would be required.
-
When will my plan become effective?
You will have a choice during the online enrollment to select the 1st or the 15th of the month for an effective date. If you select a 1st of the month effective date your initial billing will be the premium rate that was shown on the quote page. If you select a 15th of the month effective date your initial billing will be 1 ½ months premium to cover the first 45 days of your coverage. The initial billing will be processed upon submission of your application.
NEED ADDITIONAL HELP?
Give us a call or email us for any questions you may have. CLICK HERE to Send an Email
Testimonials

See What Customers are Saying About BestOne Dental!

Mike K.
Scottsdale, Arizona"Best One Dental has affordable rates, three great options to choose from and a very simple enrollment process. I love going to my dentist with only a $25 co-pay for my appointment. Since my dentist is in one of the networks the plan utilizes, I didn’t have to be involved with the claim process at all. I highly recommend this plan for anyone looking for dental coverage.”

Gilda S.
Coral Spring, Florida"I've been a member of Best One Dental for 1 year now, and I couldn't be happier with the service they provide. From routine check-ups to unexpected dental emergencies, they've consistently exceeded my expectations. Their network of dentists is extensive, making it easy to find quality care wherever I am. Plus, the claims process is seamless, with quick reimbursements and helpful customer support whenever I've had questions. I highly recommend Best One Dental to anyone looking for reliable coverage and peace of mind when it comes to dental care."
Exclusions & Limitations

For a complete listing of benefits, exclusions and limitations - please refer to your Policy. In the event of any discrepancies contained on this webpage, terms and conditions in the Policy documents shall govern. This website provides only a summary of information and the benefits and rates may vary by state.
Exclusions - This policy excludes and will not reimburse for the following services or charges.
- Services provided by anyone other than a doctor of medical dentistry or a doctor of dental surgery, unless a licensed hygienist performs the services under the direction of a doctor of medical dentistry or a doctor of dental surgery, or a denturist.
- Services received while on active duty with a military service of any country or international organization.
- Services needed because of participation in a riot or insurrection or the commission of a felony.
- Services needed as a result of a work-related injury or illness, whether or not covered under Worker's Compensation;
- Services provided by an employer.
- Services started before your effective date. Examples of excluded services under this paragraph include but are not limited to the following: obtaining an impression for an appliance, or a modification of one, before your effective date; preparing a tooth for a crown, bridge or other lab fabricated restorations before your effective date; opening a pulp chamber for root canal therapy before your effective date.
- Services not completed before your termination date.
- Services required because you failed to comply with professionally prescribed treatment.
- Telephone consultation services.
- Charges for your failure to keep a scheduled appointment.
- Services that are primarily for cosmetic reasons. Examples include alteration or extraction of functional natural teeth for the purpose of changing appearance and replacement of restorations previously performed for cosmetic reasons.
- Services for orthodontic treatment and orthodontia type procedures unless this policy defines those services as covered services.
- Services received for or related to temporomandibular joint dysfunction (TMJ).
- Charges in excess of the agreed to coverage amounts, as shown on the schedule of benefits.
- Services for correction or alteration of occlusion, or any occlusal adjustments. Expenses incurred for night guards or any other appliances for the correction of harmful habits, except as defined as a Covered Dental Expense.
- Charges for "safe fees" (e.g., gloves, masks, surgical scrubs and sterilization).
- Charges for copies of records, charts, x-rays and any other costs associated with the forwarding or mailing of these copies, or for completing dental forms.
- Charges for state or territorial taxes associated with dental services.
- Charges for services received from two or more providers for a single procedure or course of care, if those charges would have been less if received from one provider and you made the decision to transfer your care during the procedure or course of care.
- Services that are experimental or investigational.
- Services that are not within the scope of the treating provider’s practice.
- Services that are not Medically Necessary or that would not meet generally accepted standards of practice.
- Charges that you would not legally have to pay if you did not have insurance unless mandated by law.
- Services for specialized procedures and techniques, including precision attachments, personalization, and precious metal bases.
- Charges for duplicate or provisional services or supplies.
- Charges for plaque control programs, oral hygiene instruction, and dietary instructions.
- Charges for gold foil restorations.
- Charges for treatment at the hospital.
- Service to adjust a denture or bridgework within six months after it is installed or adjusted, by the same provider who installed or adjusted it.
- Charges for home health aides, including but not limited to toothpaste, fluoride gels, dental floss and teeth whiteners.
- Services to seal teeth, other than permanent molars.
- Charges to replace lost, stolen or misplaced dentures.
- Charges to repair or replace damaged, lost or missing appliances.
- Services to fabricate an athletic mouth guard;
- Charges for internal bleaching, nitrous oxide, oral sedation, and/or topical medicament centers.
- Charges for bone grafts in connection with extractions, apicoectomies or non-covered or non-eligible implants.
- Charges for a Deductible, Coinsurance, or other cost-sharing amounts for which you are responsible.
- Temporary services that are considered an integral part of a final services rather than a separate service.
- Charges for veneers and related procedures.
- Services not listed as a covered service.
- Services received outside of the United States.
- Services for or relate to the initial installation of a prosthetic device that replaces a tooth that was missing before you were covered under the policy unless such installation starts after you have been covered continuously for at least three years immediately before the date of the installation (applicable only to certain states).
Underwritten by Best Life & Health Insurance Company PO Box 19721, Irvine, CA 92623
Contact Us
Location:
8700 E Vista Bonita Dr, #174
Scottsdale, AZ 85255
Email:
info@bestonedental.com
Call:
800-454-1021
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| $23.02 | $24.86 | $42.17 | $47.65 | $44.96 |
$50.81 | |
| Individual + Spouse | $46.04 | $49.72 | $84.35 | $95.31 | $89.83 | $101.62 |
| Individual + Child(ren) | $51.79 | $55.94 | $94.89 | $107.23 | $101.17 | $114.33 |
| Family | $74.81 | $80.79 | $137.06 | $154.88 | $146.14 | $165.14 |
| MONTHLY RATES | CHOICE PLAN | |||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| Individual | $27.22 | $29.40 | $49.87 | $56.35 | $53.17 | $60.08 |
| Individual + Spouse | 54.44 | $58.79 | $99.74 | $112.70 | $106.34 | $120.16 |
| Individual + Child(ren) | $61.24 | $66.14 | $112.21 | $126.80 | $119.64 | $135.19 |
| Family | $88.46 | $95.54 | $162.08 | $183.15 | $172.81 | $195.27 |
| MONTHLY RATES | CHOICE PLAN | |||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| Individual | $25.32 | $27.35 | $46.39 | $52.42 | $49.46 | $55.89 |
| Individual + Spouse | 50.64 | $54.69 | $92.78 | $104.84 | $98.92 | $111.78 |
| Individual + Child(ren) | $56.97 | $61.53 | $104.38 | $117.95 | $111.29 | $125.76 |
| Family | $82.29 | $88.87 | $150.77 | $170.37 | $160.75 | $181.65 |
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| Individual | $15.41 | $16.64 | $30.40 | $34.35 | $32.44 | $36.66 |
| Individual + Spouse | $30.82 | $33.28 | $60.80 | $68.70 | $64.88 | $73.32 |
| Individual + Child(ren) | $34.67 | $37.44 | $68.40 | $77.29 | $72.99 | $82.49 |
| Family | $50.08 | $54.08 | $98.80 | $111.64 | $105.43 | $119.15 |
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| Individual | $18.72 | $20.22 | $36.94 | $41.74 | $39.41 | $44.54 |
| Individual + Spouse | $37.45 | $40.44 | $73.87 | $83.47 | $78.83 | $89.08 |
| Individual + Child(ren) | $42.12 | $45.49 | $83.11 | $93.91 | $88.68 | $100.23 |
| Family | $60.85 | $65.71 | $120.04 | $135.64 | $128.10 | $144.77 |
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| Individual | $16.57 | $17.89 | $32.68 | $36.93 | $34.87 | $39.41 |
| Individual + Spouse | $33.13 | $35.78 | $65.36 | $73.85 | $69.75 | $78.82 |
| Individual + Child(ren) | $37.27 | $40.25 | $73.53 | $83.09 | $78.46 | $88.68 |
| Family | $53.84 | $58.14 | $106.21 | $120.01 | $113.34 | $128.09 |
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| Individual | $18.95 | $20.47 | $37.39 | $42.25 | $39.90 | $45.09 |
| Individual + Spouse | $37.91 | $40.93 | $74.78 | $84.50 | $79.80 | $90.18 |
| Individual + Child(ren) | $42.64 | $46.05 | $84.13 | $95.07 | $89.78 | $101.46 |
| Family | $61.60 | $66.52 | $121.52 | $137.32 | $129.68 | $146.55 |
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| $14.01 | $15.13 | $27.64 | $31.23 | $29.49 |
$33.33 | |
| Individual + Spouse | $28.02 | $30.25 | $55.27 | $62.45 | $58.98 | $66.65 |
| Individual + Child(ren) | $31.52 | $34.04 | $62.18 | $70.26 | $66.35 | $74.99 |
| Family | $45.53 | $49.16 | $89.82 | $101.49 | $98.85 | $108.32 |
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| $16.79 | $18.13 | $33.11 | $37.41 | $35.33 |
$39.93 | |
| Individual + Spouse | $33.56 | $36.25 | $66.22 | $74.82 | $70.66 | $79.85 |
| Individual + Child(ren) | $37.76 | $40.78 | $74.49 | $84.17 | $79.50 | $89.84 |
| Family | $54.54 | $58.89 | $107.60 | $121.58 | $114.83 | $129.77 |
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| Individual | $14.64 | $15.81 | $28.88 | $32.64 | $30.82 | $34.83 |
| Individual + Spouse | $29.28 | $31.61 | $57.76 | $65.26 | $61.63 | $69.65 |
| Individual + Child(ren) | $32.94 | $35.57 | $64.98 | $73.42 | $69.34 | $78.36 |
| Family | $47.58 | $51.37 | $93.86 | $106.06 | $100.16 | $113.19 |
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| $21.14 | $22.83 | $39.06 | $44.14 | $41.58 |
$46.99 | |
| Individual + Spouse | $42.28 | $45.66 | $78.12 | $88.28 | $83.16 | $93.98 |
| Individual + Child(ren) | $47.57 | $51.36 | $87.89 | $99.32 | $93.56 | $105.73 |
| Family | $68.71 | $74.19 | $126.95 | $143.46 | $135.14 | $152.72 |
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| $17.95 | $19.39 | $42.71 | $47.65 | $44.96 |
$50.81 | |
| Individual + Spouse | $35.90 | $38.78 | $85.42 | $95.30 | $89.92 | $101.62 |
| Individual + Child(ren) | $40.39 | $41.83 | $95.44 | $100.38 | $101.17 | $107.02 |
| Family | $58.34 | $61.22 | $138.15 | $148.03 | $146.13 | $157.83 |
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| $19.75 | $21.33 | $46.39 | $52.42 | $49.46 |
$55.89 | |
| Individual + Spouse | $39.50 | $42.66 | $92.78 | $104.84 | $98.92 | $111.78 |
| Individual + Child(ren) | $44.44 | $46.02 | $104.38 | $110.41 | $111.29 | $117.72 |
| Family | $64.19 | $67.35 | $150.77 | $162.83 | $160.75 | $173.61 |
| MONTHLY RATES | ECONOMY PLAN | CHOICE PLAN | ||||
|---|---|---|---|---|---|---|
| Calendar Year Max Benefit Per Insured | $1,500 | $3,000 | $5,000 | |||
| 18-65 | 66+ | 18-65 | 66+ | 18-65 | 66+ | |
| $27.57 | $29.78 | $54.40 | $61.47 | $58.04 |
$65.60 | |
| Individual + Spouse | $55.15 | $59.54 | $108.79 | $122.92 | $116.08 | $131.18 |
| Individual + Child(ren) | $62.03 | $67.01 | $122.38 | $138.29 | $130.60 | $147.60 |
| Family | $89.62 | $96.76 | $176.79 | $199.76 | $188.65 | $213.19 |